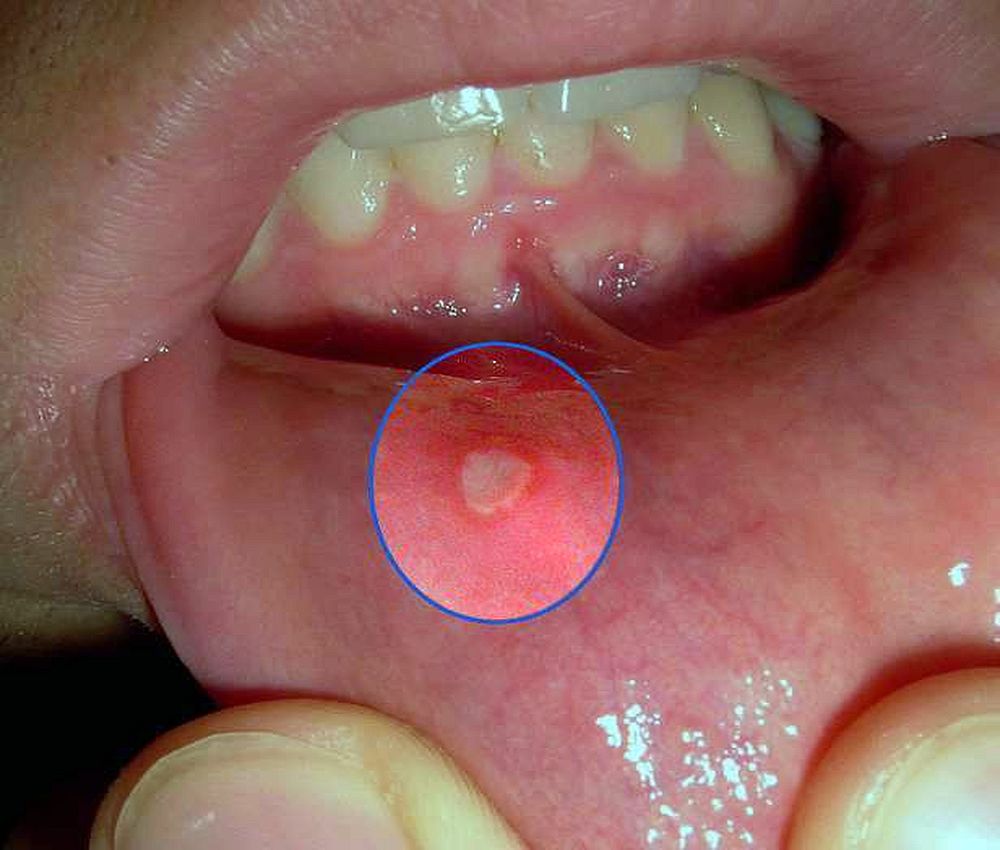
Traumatic Ulcer
Traumatic ulcers are common oral lesions. The causes are variable and include a sharp or broken tooth, rough fillings, clumsy use of cutting dental instruments, hard foodstuffs, sharp foreign bodies, biting of the mucosa, and denture irritation.
Ulcers of traumatic origin may occur anywhere in the mouth but are most commonly found on the lateral borders of the tongue, the buccal mucosa, the lips, the labioalveolar and buccalveolar grooves.
The size of the ulcer may vary from a few millimeters to several centimeters in diameter and depends on the intensity, duration, and type of the trauma as well as superimposed infection.
The clinical presentation is variable, but usually traumatic ulcers appear as single painful lesions with a smooth red or white-yellow surface and thin erythematous margins. They are usually soft to palpation and heal without scarring within 6 to 10 days, spontaneously or after removal of the cause.
However, when the cause is sustained and intense, the ulcer surface may become irregular with vegetations, the border may become raised, and the base indurated. In these cases the traumatic ulcer may clinically resemble a carcinoma.
Subjective complaints vary from mild to severe, depending on the depth and location of the ulcer in the mouth. The diagnosis is based on the history and clinical features.
► Read also: ORAL PATHOLOGY : Pemphigus Vulgaris Diagnosis
Once a relationship has been established between an ulcerogenic factor and an ulcer, removal of the cause is mandatory, with follow-up of the patient for 7 to 10 days to verify complete healing.
If the ulcer persists, then revision of the clinical diagnosis and performance of a biopsy to rule out cancer is recommended. The differential diagnosis should include squamous cell carcinoma and other cancers, syphilis, tuberculosis, aphthae, and eosinophilic and other ulcers.
Laboratory test. Histopathologic examination often helps in establishing the diagnosis.
Treatment. Removal of the traumatic factors.
Traumatic Bulla
Acute traumatic injury of the oral mucosa, usually caused by biting or prosthetic appliances, may produce abrupt subepithelial hemorrhages which sometimes detach the epithelium at the dermoepithelial junction to produce a hemorrhagic bulla formation. The buccal mucosa is the site of predilection, but rarely it may be seen in other oral areas.
The lesion is asymptomatic and usually disappears within 2-3 days without treatment. The differential diagnosis includes pemphigus, cicatricial pemphigoid, bullous pemphigoid, and epidermolysis bullosa acquisita.
Traumatic Hematoma
Traumatic hematoma of the oral mucosa occurs under the influence of mild or severe mechanical forces that result in hemorrhage within the oral tissues.
Clinically, it appears as an irregular lesion with a deep red hue. The most common sites of hematoma are the tongue and lips and the most common causes are biting of the oral mucosa or careless use of dental instruments.
Chronic Biting
Mild chronic biting of the oral mucosa is common in anxious persons. These patients consciously bite the buccal mucosa, tongue, or lips and tear off the superficial epithelial layers.
Clinically, this lesion is characterized by a diffuse irregular area of small furrows, whitish surface, and desquamation of the affected epithelium. Infrequently, there are surface erosions and petechiae.
The differential diagnosis includes leukoedema, Fordyce's granules, candidosis, leukoplakia, white sponge nevus, and lichen planus. Treatment includes mild sedatives and warning the patient about the deleterious results of this habit on the oral mucosa.
Toothbrush Trauma
Toothbrush trauma may occur during aggressive tooth-brushing with a hard brush. The clinical picture consists of small oval, round, or bandlike superficial erosions located on the gingiva and alveolar mucosa. These lesions cause mild subjective complaints and heal rapidly.
The differential diagnosis includes herpes simplex, aphthous ulcers, and other traumatic lesions.
Denture Stomatitis
Denture stomatitis or denture sore mouth is frequent in patients who wear dentures for long periods of time. Usually, the lesion is confined to the maxilla and only rarely occurs on the mandibular mucosal surface.
Clinically, the mucosa beneath the denture is edematous, red with or without whitish spots that represent accumulation of hyphae of Candida albicans, or food remnants. The mucosal surface is smooth or granular.
Most patients are asymptomatic but some complain of a burning sensation or irritation and pain.
The lesions are benign and may be localized or generalized. The most important causative factors of denture stomatitis are irritation from the denture, food debris accumulating under the denture surface, and C. albicans infection.
The differential diagnosis includes allergic contact stomatitis due to acrylic.
Treatment. Improvement of denture fit, good oral hygiene, and nystatin or clotrimazole if C. albicans is present.
°saudedireta.com.br
°George Laskaris, D. D. S. , M. D
Disqus comments